Can exercise really prevent cancer?
Gillian White – BSc, MSc. PhD (C)
Faculty of Kinesiology and Physical Education, University of Toronto; Department fo Physiology and Experimental Medicine, Hospital for Sick Children, Toronto, Ontario, Canada.
Over the last decade, it has become increasingly clear how important exercise is for not only general health and fitness but also prevention of chronic and life-threatening diseases. Exercise has been shown to act as both a prevention and treatment for diseases responsible for leading mortality and morbidity rates including cancer, heart disease, stroke, diabetes, osteoporosis, and metabolic disorders. In this article, we focus on the recent research behind the importance of exercise in prevention of cancer and the protective effects exercise has on the body.
What is Cancer?
Cancer is a disease of the cell’s genetic material that informs how the cell grows and divides. While “Cancer” is a common name for thousands of individual variations of disease, all cancers share common traits. Mutations to DNA can occur through random mutation (mistakes during replication), damage by internal toxins (i.e. free radicals), or damage by external toxins (radiation/sun, chemicals, etc.). In healthy cells, these mutations are noticed and corrected or if the mistakes/mutations are too substantial, the cell undergoes programmed/controlled cell death. If these systems aren’t working right or miss a mutation, the cell can be detected by the immune system and cleared. The development of cancer tends to be a double edged sword of increased mutations and weaker function of repair/detection systems. Over time, more mutations the cell’s regulation of growth and division (proliferation) is altered such that the cells have increased or more sensitive responses to “grow” signals (or make their own grow signals), decreased sensitivity to “stop” signals, a lower capacity to repair damaged DNA. This results in cells that grow too fast but are also not functional because of the DNA damage that they’ve sustained. Eventually these dysfunctional cells with an advantage in growth over healthy cells build a mass that takes over whatever function the tissue it originated in, forming a tumour. The symptoms of the specific cancer type reflect loss of function or pain in the tissue that the tumour has developed in.
For cells to acquire the necessary random mutations to become cancerous without being detected by the body’s immune system or by systems in the cell that recognize DNA replication errors or abnormal growth/proliferation, it takes a lot of random mutations in the right order. Imagine a million monkeys on a million type-writers hammering out Shakespeare by pure probability – it takes the right random key strokes in the right random order –probability is on the side of these cells being noticed and discarded by the body. The body has these check systems in place both within the cells (DNA repair systems) and within the body (immunosurveillance) to not let cells with mistakes in DNA replicate or remain in the tissue. So it’s not surprising that cancer rates increase with age – probability wise, the monkeys have had more time to make more random key strokes (and if there was a supervisor monkey looking for errors and tossing out bad scripts, that monkey is tired from reading random errors for decades).
How can the immune system prevent/fight cancer?
If mutations have occurred to the genes controlling the repair systems internally, a strong immune system is paramount to clearing any potentially cancerous or pre-cancerous cells from remaining in the body to develop into full out cancer. The immune system is comprised of two arms: the innate system notices cells that aren’t ours or that have been corrupted (but virus or like tumour/mutated cells) and attacks them upon random encounter. This system works immediately but depends on having enough cells in circulation to come into contact with these “non-self” or “corrupt” cells to outnumber and effectively eliminate them. A number of different types of cells are a part of the innate immune system but one of the most important types are called Natural Killer cells. The adaptive immune system has the ability to recognize and remember what a particular “non-self” or “corrupt” cell looks like, and can then create clones of these cells that recognize and remember what these target cells look like. The creation of clones to take out the target cells give a numbers advantage to the adaptive immune system. This cloning/proliferation of immune cells occurs in lymph nodes where yet-to-be activated immune cells hang out. Again, a number of different cells comprise the adaptive immune system but, as far as cancerous or pre-cancerous cells go, the important effector cells of this system at Thymic cells (T-cells). The two arms of the immune system work together so the NK cells first notice the tumour cells and start to fight them to keep tumour cell numbers at bay but then send a messenger cell (dendritic cell) that knows what these corrupt cells look like to the lymph nodes to show the naïve T-cells what they’re looking for. An army of T-cells is then produced in the lymph nodes and released into the blood to travel to the tumour where they take over the fight from NK cells.
For this coordinated attack on tumour cells to occur, signalling between the cell types must occur to act to tell the army where they are needed, stimulate fighting power, cut off blood and nutrient supply to tumour cells, and effectively destroy the impending tumour. This occurs through hormones and cytokines (signalling molecules released from immune cells and damaged/stressed cells) directing traffic and stimulating fighting power.
How does exercise prevent cancer?
Exercise can act in two ways to prevent cancer: 1. Reduce mutation frequency by increasing anti-oxidant status (anti-oxidants neutralize free radicals which are responsible for DNA damage and mutations). 2. Promote immune health and immunosurveillance to effectively detect and destroy tumour cells. The theory of immunosurveillance has been around since the early 1900s and was popularized in the 70s (Ichim 2005). This theory is supported by findings showing immunosuppression by carcinogens, higher risk of certain cancer types in immunosuppressed individuals (i.e. post organ transplant, HIV) (Ichim, 2005, Dunn et al 2002), and epidemiological studies showing lower cancer rates in people who report higher levels of physical activity (Walsh et al, 2011). We know exercise is good for your health but it hasn’t been until recently when the relationships between the immune system and cancer and exercise and the immune system have become more clear that we can actually start to understand what is happening during exercise that is preventing the development of cancer.
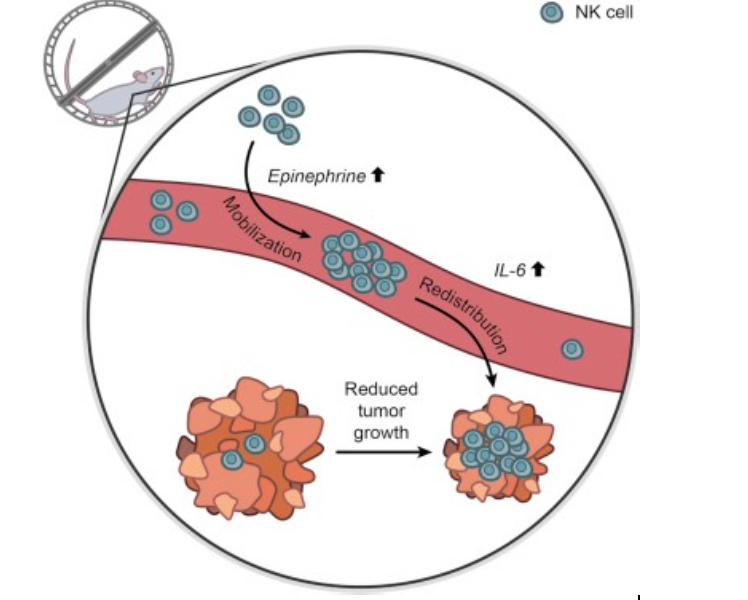
A recent study out of Copenhagen by Pedersen et al. induced melanoma in rats and either had them exercise on a running wheel or remain sedentary. After months of this treatment, they found that the rats that exercised had lower growth of tumours, lower metastasis (spread) of tumours, and overall lower development of the cancer they had induced. To understand what effect exercise was having that could account for these findings, the authors also looked at blood samples and observed higher levels of adrenaline, NK cells, and an important signalling molecule Interleukin-6 (IL-6). While these findings themselves are interesting, they don’t fully paint the picture of how exercise is affecting tumour development or if these changes in the blood have a causal effect between exercise and tumour development. To uncover these queries, they did a second study replicating the first, but blocking the release of adrenaline (also called “epinephrine”) during their running wheel exercise and found that this negated any anti-tumour effect of exercise.
So what is it about adrenaline release during exercise that results in health promotion and prevention of serious illness like cancer? Adrenaline is released during exercise in proportion to how stressful the exercise is for your body (how intense is was, how long you went etc.). When adrenaline is released it increases the number of NK cells in your blood stream – aka. the number cruising around looking for rogue cells in the body. Exercise also causes increased IL-6 in the blood that stimulates the circulation and function of immune cells. Adrenaline and IL-6 are both increased during stress and injury, which have both been associated with negative health outcomes. What differentiates exercise from stress or injury is that it is acute – that is to say, it only lasts 1-2 h and is then followed by opportunities to rebuild for the next bout (with hydration, nutrition, sleep etc.). That makes the stress systems stronger and more responsive for the next bout of stress so when a foreign pathogen/virus comes along or mutated cells develop in a tissue, your body can wipe it out quickly and effectively before it grows/spreads into something potentially life threatening.

Figure 1. The mechanism suggested by Pedersen et al. in their recent article published in Cell Metabolism. Exercise increased epinephrine (adrenaline) and interleukin-6 (IL-6), which enhance the responsiveness of immune cells’ mobilization and redistribution to sites where tumours are growing. The immune cells then act to eliminate tumour cells, resulting in reduced progression of the tumours in mice that exercise compared with those that were sedentary. Taken from Pedersen et al., 2016.
Tying it all together
Your immune system can recognize both cells/viruses that are pathogenic invaders as well as cells that are ours but have been damaged. Coordination between the innate and adaptive immune systems recognizes and eliminates these threats to our health and exercise promotes the responsiveness and robustness of these systems by acting as a stress for a short period of time. Short bursts of stress promote adaptation to strengthen systems keeping not only our muscles and body strong, but also our immune system to keep us both fit and healthy.
What kind of exercise is best to promote immune health?
While all of this is very interesting, what does it mean for our Fast Twitch Granmas out there? Regular, moderately-high intense (~60%-75%VO2max or 50-80% heart rate reserve, 45min – 1 h) aerobic exercise is known to:
Increase anti-oxidant status – potentially reducing ROS damage to DNA and subsequent mutations (Rogers et al., 2008)
Reduce chronic inflammation – Expected to maintain innate and adaptive immune cell responsiveness to pathogenic or tumour-antigenic challenge (Dhabhar, 2014; Rogers et al., 2008).
Increased NK numbers and function – Shown to be increased with regular moderate exercise (Kruijsen-Jaarsma et al., 2013; Rhind et al., 1994).
T cell function – Shown to be increased lymphocyte subsets have been observed after moderate intensity aerobic exercise programs.
Better energy balance – Reduced energy balance (in favour of energy expenditure), influenced by metabolic demands of exercise, reduces cancer risk (Shephard & Shek, 1995).
References:
Dhabhar, F. S. (2014). Effects of stress on immune function: the good, the bad, and the beautiful. Immunologic Research, 58(2-3), 193–210.
Dunn, G. P., Bruce, A. T., Ikeda, H., Old, L. J., & Schreiber, R. D. (2002). Cancer immunoediting: from immunosurveillance to tumor escape. Nature immunology, 3(11), 991–998.
Ichim, C. V. (2005). Revisiting immunosurveillance and immunostimulation – implications for cancer immunotherapy. Journal of Translational Medicine, 3(1), 8.
Kruijsen-Jaarsma, M., Révész, D., Bierings, M. B., Buffart, L. M., & Takken, T. (2013). Effects of exercise on immune function in patients with cancer: a systematic review. Exerc Immunol Rev, 19, 120–143.
Pedersen, L., Idorn, M., Olofsson, G. H., Nookaew, I., Hansen, R. H., Johannesen, H. H., … Hojman, P. (2015). Exercise suppresses tumor growth through epinephrine- and IL-6-dependent mobilization and redistribution of NK cells. Journal for Immunotherapy of Cancer, 3(Suppl 2), P246.
Rogers, C. J., Colbert, L. H., Greiner, J. W., Perkins, S. N., & Hursting, S. D. (2008). Physical activity and cancer prevention : pathways and targets for intervention. Sports medicine (Auckland, N.Z.), 38(4), 271–296.
Rhind, S. G., Shek, P. N., Shinkai, S., & Shephard, R. J. (1994). Differential effects of Interleukin-2 Receptor Alpha and Beta chains in relation to Natural Killer cell subsets and aerobic fitness. Int J Sports Med 15, 911-918.
Shephard, R. J., & Shek, P. N. (1995). Cancer, immune function, and physical activity. Canadian Journal of Applied Physiology/Revue Canadienne de Physiologie Appliquee, 20(1), 1–25.
Walsh, N. P., Gleeson, M., Shephard, R. J., Gleeson, M., Woods, J. A., Bishop, N. C., Fleshner, M., Green, C., Pedersen, B. K., Hoffman-Goetz, L., Rogers, C. J., Northoff, H., Abbasi, A., & Simon, P. (2011c). Position statement. Part one: Immune function and exercise. Exerc Immunol Rev, 17, 6–63.









